Migraine and pregnancy: how to plan, what to treat safely
Many women suffering from migraines are afraid to plan a pregnancy. These fears are justified - judging by the instructions, 99% of medications cannot be taken while pregnant. However, a review of studies on migraine in pregnancy found that there are treatment options.
Good news: up to 80% of women experience relief from attacks already in the first trimester (especially among the group with menstrual migraines), up to 60% forget about it until the end of breastfeeding. For 4-8% of expectant mothers, a miracle does not happen; it was for them that I conducted my research.
Information on sources and literature is included at the end of the article with detailed commentary.
Does migraine affect pregnancy?
Potential problems are possible and should be known in advance. But, if we are attentive to ourselves and collect a small amount of knowledge, it will be easier to survive this period.
Severe attacks with an aura that last longer than a day and continue into the second and third trimester can cause anxiety. Such conditions can provoke preeclampsia and some other complications (in the article I do not want to write any frightening statistics, but I must indicate the source for independent study [1]( https://www.ncbi.nlm.nih.gov/pubmed/ 29052046)).
Migraine does not directly affect the fetus. However, the child is indirectly harmed by the mother’s poor health, lack of sleep and fasting during severe attacks. Low baby weight is the most common negative impact of the disease. Therefore, in severe cases, you need to try to stop the attack, and not try to endure it.
What symptoms should alert the expectant mother
Some migraine symptoms, especially those appearing for the first time, may be a reason to consult a doctor (urgently):
- This is the first time you have experienced an aura or it lasts longer than an hour;
- High blood pressure (always measure, even when you think that a typical attack is coming);
- The pain came suddenly and reached maximum intensity within 1 minute;
- The temperature has risen, the neck muscles are in spasm (you need to call a joint venture);
- Simultaneous fear of light and sound;
- The headache is not one-sided, but just as strong and throbbing;
- Change in the nature of pain;
- The first attack comes at the end of the second or third trimester.
The doctor will carefully evaluate atypical manifestations and rule out other diseases, and may prescribe further examination.
How to relieve a migraine attack in pregnant women
For ethical reasons, pregnant women are not allowed to participate in any controlled drug trials. Therefore, in the instructions for the vast majority of medications, pregnancy is a contraindication for use - we cannot directly prove safety. But this does not mean at all that “everything is impossible.”
. The original and translation are in the appendix at the end of the article.") Tablets adapted from Nature Reviews Neurology 11, 209–219 (2015). The original and translation are in the appendix at the end of the article.
Tablets adapted from Nature Reviews Neurology 11, 209–219 (2015). The original and translation are in the appendix at the end of the article.
We have access to therapeutic and clinical observations that are included in special registries in all developed countries. Based on the results of systematic reviews of data from such registries, doctors draw conclusions about the safety of drugs.
This article is the result of studying several dozen recent reviews.
I’ll start with heavy artillery. A wary attitude still remains towards the serotonin 5-HT1 agonists - triptans. However, application experience is accumulating and more and more encouraging data are emerging.
Triptans
This is a relatively young class of drugs, but all migraine sufferers are familiar with them, as they are the “gold standard” of treatment. The most studied is sumatriptan, approved for use in 1995 - the clinical history of the substance is 20 years.
Of the eight triptans currently used, it has the least pronounced vasoconstrictor effect and does not cause uterine contractions. Sumatriptan can be considered a relatively safe therapeutic alternative for pregnant women experiencing worsening migraine in the first trimester.
There is more and more clinical data, and it does not show a negative effect of sumatriptan on the course of pregnancy and the health of the child. However, for women with a history of migraine, there is always a statistically significant number of newborns weighing less than 2500 g (both those who took the drug and those who did not).
Literally before the publication of the article, I found the latest British medical manual , which contains sumatriptan in the recommendations with the note: “no adverse outcomes were identified, it can be recommended” .
Not so long ago they began to conduct research on a living placenta: no more than 15% of a single minimum dose overcomes the barrier. This amount of the substance does not have any effect on the fetus 2 . Prenatal use should be discontinued as the substance may increase the risk of postpartum haemorrhage. This is directly related to its mechanism of action.
The largest studies of AC5-HT1 are carried out by Norwegians, Swedes and Danes. They have phenomenal medical registries that document everything. I recommend that you read the Norwegian review, as it contains a number of valuable information that cannot be included in the article 3 .
Nonsteroidal anti-inflammatory drugs (NSAIDs)
Ibuprofen, naproxen and diclofenac are considered relatively safe choices in the second trimester, but are not recommended in the first and third trimesters. Ibuprofen should be avoided after 30 weeks due to an increased risk of premature closure of the ductus arteriosus and oligohydramnios. Some population-based studies support problems with NSAIDs in the first trimester, others do not.
 The conclusion of a meta-review of all studies on ibuprofen for migraines shows that it is on average 45% more effective than placebo.
The conclusion of a meta-review of all studies on ibuprofen for migraines shows that it is on average 45% more effective than placebo.
Taking NSAIDs interferes with conception and seriously increases the risk of miscarriage.
Aspirin in minimal doses can be taken until the third trimester, no later than 30 weeks (no more than 75 mg per day), if it led to relief of migraines before pregnancy. If aspirin did not help, there is no point in taking risks, since it affects the baby’s platelet function.
Analgesics
Paracetamol (acetaminophen) is the drug of choice for pain relief during an attack. It is most effective in combination with aspirin and caffeine (our Citramon or Citrapak). In this case, caffeine acts as a transport, helps the absorption of substances, and its amount in the tablet does not have any stimulating effect. It is necessary to remember about the restrictions on taking acetylsalicylic acid.
The Journal of Headache and Pain (2017) 18:106 page 11 states: “Based on the above data, paracetamol 500 mg or in combination with aspirin 100 mg, metoclopramide 10 mg or tramadol 50 mg is recommended as the first choice of symptomatic treatment heavy attacks.”
Some women stop an attack with paracetamol if they manage to take it in the first minutes after the aura “turns on.”
 Acetaminophen or paracetamol
Acetaminophen or paracetamol
A large Danish study found a statistically significant increase in hyperactivity in babies whose mothers took at least 2 doses of paracetamol per week during pregnancy. Other reviews do not find similar correlations. Of course, dosage and frequency of administration are critical.
Caffeine
There are lucky women who can significantly relieve migraine pain with a cup of coffee. Sometimes even I can do this trick. Coffee is the simplest and safest way to help yourself during an attack. There is no evidence of a negative effect of household doses of caffeine on pregnancy and the fetus (2 cups per day). If caffeine helped before, you shouldn’t give it up now.
Opiates and opioids
Only weak ones, such as tramadol and codeine. One or two doses are allowed for the entire prenatal period, if none of the above has given results. Plant-based opioids are rare, but sage tea should be avoided (in addition to containing opiates, it is believed to cause uterine contractions).
Even if tramadol relieved pain well before pregnancy, try other options. Most likely, during this period, opiates will increase nausea and there will be no point in taking them at all. Although I very well understand migraineurs who hold tightly to what first helped. The main problem is chronic pain, which quickly gets worse while taking opiates. Over time, there will be nothing to stop the attacks.
Antiemetics
Metoclopramide and cyclizine are sometimes prescribed for severe toxicosis, and the equally effective domperidone has not yet been sufficiently studied. An antiemetic significantly relieves migraine symptoms and increases the likelihood that the drug itself will work (it is recommended to take it together with sumatriptan) [4]( https://www.ncbi.nlm.nih.gov/pubmed/?term=Sumatriptan+plus+metoclopramide+in+triptan -nonresponsive+migraineurs).
 Metoclopramide
Metoclopramide
Chlorpromazine and prochlorperazine strictly until the third trimester. Doxylamine, histamine H1 receptor antagonists, pyridoxine, dicyclomine and phenothiazines have not been reported to cause adverse effects on the fetus or pregnancy, but are prescribed much less frequently than metoclopramide. The problem with antiemetics is side effects, avoid systematic use.
Preventive treatment of migraine in pregnant women
The group of preventive measures includes medications, dietary supplements (dietary supplements) and some physical therapy: massage and acupuncture. I won’t swear about acupuncture here, besides, as part of placebo psychotherapy, it helps specifically with pain and anxiety disorders ( Acupuncture for the prevention of episodic migraine ). I looked through several British manuals - not a word about acupuncture, it’s already nice.

Medicines
Almost everything that is usually recommended for migraine prevention is not suitable for expectant mothers: beta blockers, antiepileptics, antidepressants, ACEs, ARBs, calcium channel blockers and the as yet little studied botulinum toxin type A (BTX-A).
All this is used to treat hypertension, depression and epilepsy. We do not prescribe such drugs to ourselves, therefore, when planning a pregnancy, you need to ask your doctor questions about reducing doses or the possibility of temporarily discontinuing some drugs from these groups.
Beta blockers
With antihypertensive drugs such as metoprolol and propranolol, things are complicated. Most evidence suggests that you should gradually stop taking them before conception.
Propranolol has a strong evidence base for the prevention of migraine and in some cases it is necessary in hypertensive patients, including pregnant women. Then its reception continues in the minimum possible dose strictly until the second trimester.
Lisinopril, enalapril and other drugs are strictly prohibited. Verapamil remains the drug of choice at a minimal dose (1). All beta blockers are discontinued until the third trimester.
Antiepileptic drugs
Valproate and topiramate are very effective, but are prohibited during preparation for conception and pregnancy. There is no doubt about the teratogenicity of these drugs. Lamotrigine for the treatment of bipolar disorder is sometimes prescribed for migraines, and although the drug has a good safety profile in pregnancy, it is no better than placebo ([Antiepileptics for the prophylaxis of episodic migraine in adults](http://cochranelibrary-wiley. com/doi/10.1002/14651858.CD010608/abstract)).
Antidepressants
The use of the most appropriate tricyclic antidepressant Amitriptyline is considered safe (10-25 mg per day 6 ). Its negative effect on pregnancy and the fetus has not been proven, but there is evidence of an increased risk of preeclampsia in women with depression who take it systematically.
However, amitriptyline has been suggested as a second-line choice after beta-blockers as a preventative measure. By the thirtieth week, any antidepressants are gradually discontinued.
Dietary supplements
Complementary (the same alternative) medicine is not the best solution when looking for safe ways to relieve a severe attack. But some of the usual safe substances that are not drugs can help in prevention.
Magnesium
Has level B in terms of proven effectiveness for migraine prevention (literally: Level B: Medications are probably effective). Safe during pregnancy (exception: intravenous administration for more than 5 days may affect the formation of the baby’s bone tissue).
While studying the material for this article, I found the latest meta-review of research on magnesium in migraine therapy (2018) 7 . Magnesium citrate (citrate) remains the most bioavailable (600 mg recommended dosage), the worst is the oxide. The site has a separate article devoted to the treatment of migraines with magnesium, which I will supplement with the latest data.
There is only one condition - magnesium works if there is a deficiency in cells. Nevertheless, it is worth trying if you have a choice between a dietary supplement and heavy artillery.
Pyridoxine (Vitamin B6)
Reduces the number of attacks and significantly dulls nausea. Pyridoxine has been shown to be safe during pregnancy at very high doses in animals and has been approved by the FDA. The exact mechanism of action is not fully understood, more details about this in the source. There are specific dosage recommendations: 80 mg B6 per day or in combination with other supplements 25 mg per day (for example, folic acid/B12, or B9/B12).
Pyrethrum (Tansy Maiden)
A new substance with conflicting data on both efficacy and safety. Known more for the purified version of MIG-99. There is a risk of uterine contractions while feverfew is not in the recommendations of recent reviews.
Coenzyme Q10
Level C: effectiveness not confirmed, but possible. There is evidence for the prevention of preeclampsia, so it is recommended as a dietary supplement (for some reason, it is especially recommended by the Canadian Headache Society).
Riboflavin (Vitamin B2)
Level B. Everyone knows it as a prophylactic for iron deficiency anemia. There is a recommended dosage for treating migraines with riboflavin: 400 mg per day. For expectant mothers, the dosage may vary.
Melatonin
Based on several studies (no reviews yet), melatonin is safe and effective for treating migraines in pregnant women. The bioavailability of melatonin from drugs is still a big question. However, several small placebo-controlled studies have shown statistically significant results compared with placebo and amitriptyline in preventing attacks 8 . If you have problems with sleep or circadian rhythms, why not try melatonin - it may be an alternative to antidepressants 9 .
Nerve blockade with anesthetic injections
A method used in hopeless cases, with refractory migraine. The procedure is an alternative to combinations of anticonvulsants + antidepressants + opioids. Peripheral nerve blocks are not uncommon now, but they are avoided in pregnant women. The West is accumulating more and more data on the blockade in pregnant women, the results are more than optimistic 10 . In some cases, attacks do not return for up to six months.
Injections are given at one or more sites: greater occipital nerve, auriculotemporal, supraorbital and supranuclear nerves (1-2% lidocaine, 0.5% bupivacaine or corticosteroids). Pain relief is immediate in 80% of cases. For a small percentage of people it doesn’t help at all.
The procedure is better known as an occipital nerve block. Lidocaine is safe, bupivacaine is moderately safe (less data), and topical steroids are still under debate. Of all the treatments for chronic headaches, lidocaine blockade is the most promising in the context of pregnancy.
Conclusions. Careful consideration should be given to the choice of medications already at the planning stage. It is especially important to resolve the issue with prophylactic medications that we take regularly - almost all prophylaxis is gradually stopped even before conception. A little extra knowledge won’t hurt, even if you have complete confidence in your doctor.
How to treat migraine during breastfeeding
The lactation process protects up to 80% of women from migraines. If the attacks return, it is much easier to control the condition during this period than during pregnancy. It is enough to know the concentration of the drug in milk and its ability to be absorbed by the baby 12 .
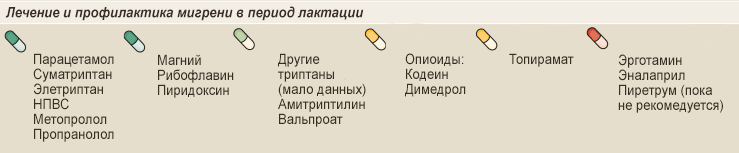
Paracetamol is considered the safest during breastfeeding. The concentration in breast milk is low, and the metabolism of babies is approximately the same as that of adults. In the entire history of clinical observations, there is one known case of a rash in a newborn (2 months) after exposure to paracetamol through mother’s milk.
NSAIDs are compatible with breastfeeding, ibuprofen is recommended as the drug of choice due to its short half-life (approx. 2 hours). Excretion in GM is low and no side effects have been reported. Diclofenac and naproxen should be taken with caution, feeding after 4 hours. These are the drugs of the second group of choice.
Irregular single doses of aspirin are acceptable, but in general, controversy surrounding acetylsalicylic acid continues. The substance has a high level of excretion and affects the baby’s platelets.
Triptans, even injectable ones, almost never pass into mother’s milk. But the conservative precautionary measure (in force since 1998) has not yet been abolished - a 12-hour break between intake and feeding. Given sumatriptan’s half-life of approximately 1 hour and extremely low bioavailability, 12 hours is excessive. Most current research recommends resuming feeding after recovery from the attack.
Eletriptan has been little studied during pregnancy, but for the lactation period it is preferable to sumatriptan. The fact is that the substance is bound by plasma proteins and practically nothing reaches the GM. The complete safety of a dose of 80 mg eletriptan per day has been assessed 11 .
Opioids are acceptable as emergency one-time aid, as they have a low concentration. We are always talking only about codeine, it is the weakest of all narcotic painkillers.
 Codeine
Codeine
Ergotamine (ergot alkaloid) is not allowed at all. This drug is very weak, and its side effects cause more problems than relief. Extremely high accumulation in milk, leading to cramps and dehydration.
Antiemetics, in particular metoclopramide, have excretion slightly above average (it is unstable and depends on the mother’s body: from 4.7 to 14.3%), but is not systematically allowed during breastfeeding. No side effects were reported in children.
Beta blockers can be returned after delivery. Most reviews agree on the most studied drugs being metoprolol and propranolol. The excretion of compounds into breast milk is low, up to 1.4% of the metabolized maternal dose, which is a negligible amount even for preterm and low birth weight infants. This is good news because some medications need to be taken regularly.
Anti-epileptic, prohibited during pregnancy, are allowed during lactation. Valproate almost does not reach the GM - 1.7% max., only trace amounts are found in the child’s plasma. Topiramate gives a concentration of up to 23%, and despite the fact that it is considered compatible with breastfeeding, monitoring is necessary in very young children: irritability, weak sucking reflex, diarrhea.
Antidepressants, particularly amitriptyline, can be used as migraine prophylaxis when first-line medications (beta blockers and dietary supplements) do not work. Compatible with breast milk, the level of the substance in milk is low - up to 2.5% of the mat. doses. The child’s plasma level is below detectable or trace levels. Other antidepressants are not considered, since their half-lives are much longer and they can theoretically accumulate in the baby’s body (there is no data as such).
Prils, enalapril in particular, are nephrotoxic to newborns. Their excretion is extremely low - up to 0.2%, but given that enalapril is taken daily, it is considered incompatible with breastfeeding. Some sources say to take “with caution and control.”
Magnesium and riboflavin can be taken additionally. Their quantity in GM increases slightly.
Conclusions. All effective drugs for the treatment of severe migraines are compatible with breastfeeding, since they are not transferred into mother’s milk in pharmacologically significant quantities. Having read dozens of reviews and studies, I have never come across any recommendations about pumping, but this choice always remains with the mother.
Sources and literature
I would like to draw attention to the sources of information. All articles and meta-reviews I reference were published in peer-reviewed clinical journals. The most important and recent materials are placed in a separate folder on Google Drive with free access.
You have the opportunity to familiarize yourself with the original source; the documents contain:
- Full texts in the original, downloaded from sci-hub (with footnote numbers assigned in the article (1-11) and links to them).
- Machine translation of each original article and review that I link to (but without tables, they are very difficult to translate and format).
The original materials contain a lot of useful information about different types of headaches in pregnant women; not everything can be fit into one article. I always recommend turning to the original source, even if you trust the author of the Russian-language text. You may find instructions useful for searching for medical information.
I hope the work done will be useful to someone.



